Initial Maternal and Fetal Assessment
exp date isn't null, but text field is
#1 cause of non-obstetric death in pregnancy= trauma with 6-7% maternal mortality, as high as 60-80% fetal mortality. Affects 7% of all pregnancies, 50% occur during 3rd trimester. Etiologies are 50% MVC, 22% falls, 22% assault, 2% other. Treat mother 1st and fetus 2nd.
Consider physiologic changes of pregnancy:
- ↑ blood volume/HR/CO; ↓ SVR/BP (hypervolemia leads to delayed signs of shock)
- ↑ TV/MV; ↓ FRC/PaCO2
- ↑ RBF/GFR; ↓ BUN/Cr
- ↑ GI motility; ↓ GB emptying
- ↑ WBC volume/hypercoaguability; ↓ RBC volume
Concerning obstetric signs:
- vaginal bleeding, ruptured membranes, bulging perineum, contractions, and abnormal fetal heart rate/rhythm
Obstetric complications:
- uterine rupture, placental abruption, fetomaternal hemorrhage/Rh incompatibility, and amniotic fluid embolism
Level 1 Recommendations
- None
Level 2 Recommendations
- All pregnant pts > 12 wks gestation (GA) should have Kleihauer-Betke analysis
- 72 hr window to prevent alloimmunization; Rh immune globulin dose is 300 mcg per 30 ml fetomaternal hemorrhage
- All pregnant pts > 20 wks GA should have cardiotocographic monitoring for > 6 hrs. Continue evaluation/monitoring for uterine contractions, a non-reassuring fetal heart rate pattern, vaginal bleeding, significant uterine tenderness, serious maternal injury, or rupture of the amniotic membranes.
Level 3 Recommendations
- Best initial treatment for fetus is resuscitation of mother and early fetal assessment
- All female pts of childbearing age with significant trauma should have β-HCG and be shielded for all X-rays except pelvic/lumbar imaging.
- Concern for radiation exposure should not prevent medically indicated maternal diagnostic studies, however alternatives should be considered when possible
- Exposure <5 rad has not been associated with an increase in fetal anomalies or pregnancy loss and is therefore deemed safe at any gestational age.
- US/MRI is not associated with known adverse fetal effects, however MRI not recommended in 1st trimester due to limited experience
- Consult radiology to calculate estimated fetal dose when multiple X-rays performed
- Perimortem cesarean section should be considered in any moribund pregnant pt ≥ 24 wks GA, should ideally start within 4 min of maternal arrest, must occur within 20 min of maternal death
- Tilt left side down 15o to prevent supine hypotension syndrome
- Consult OB for all trauma in pregnancy
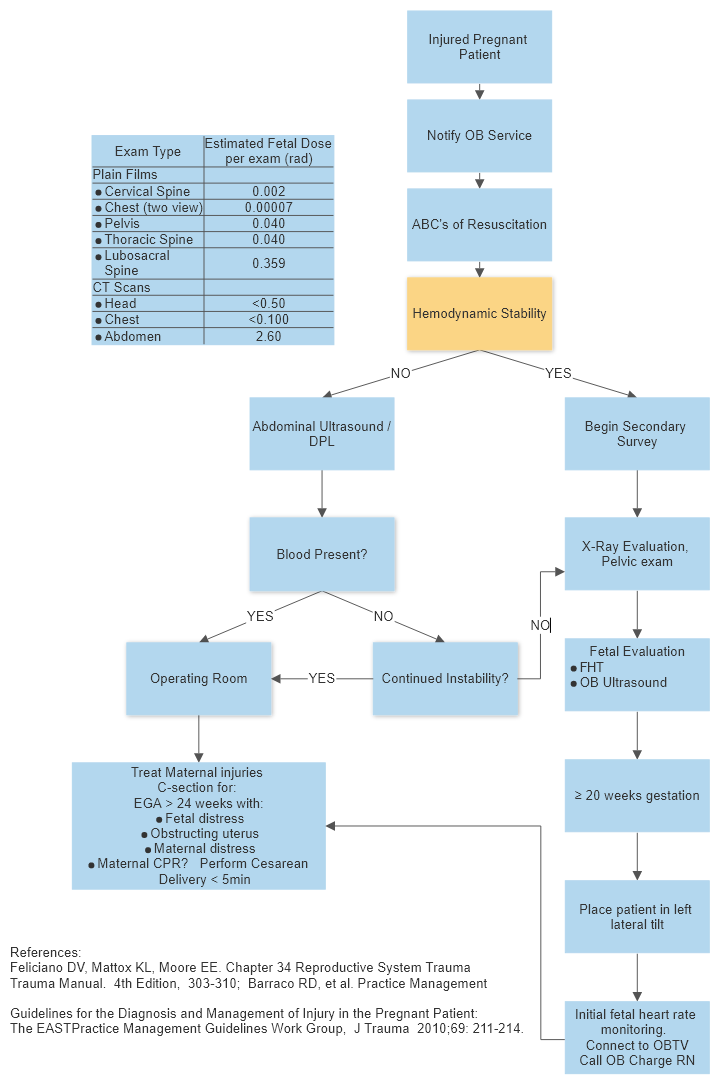
Algorithm for Initial Maternal and Fetal Assessment