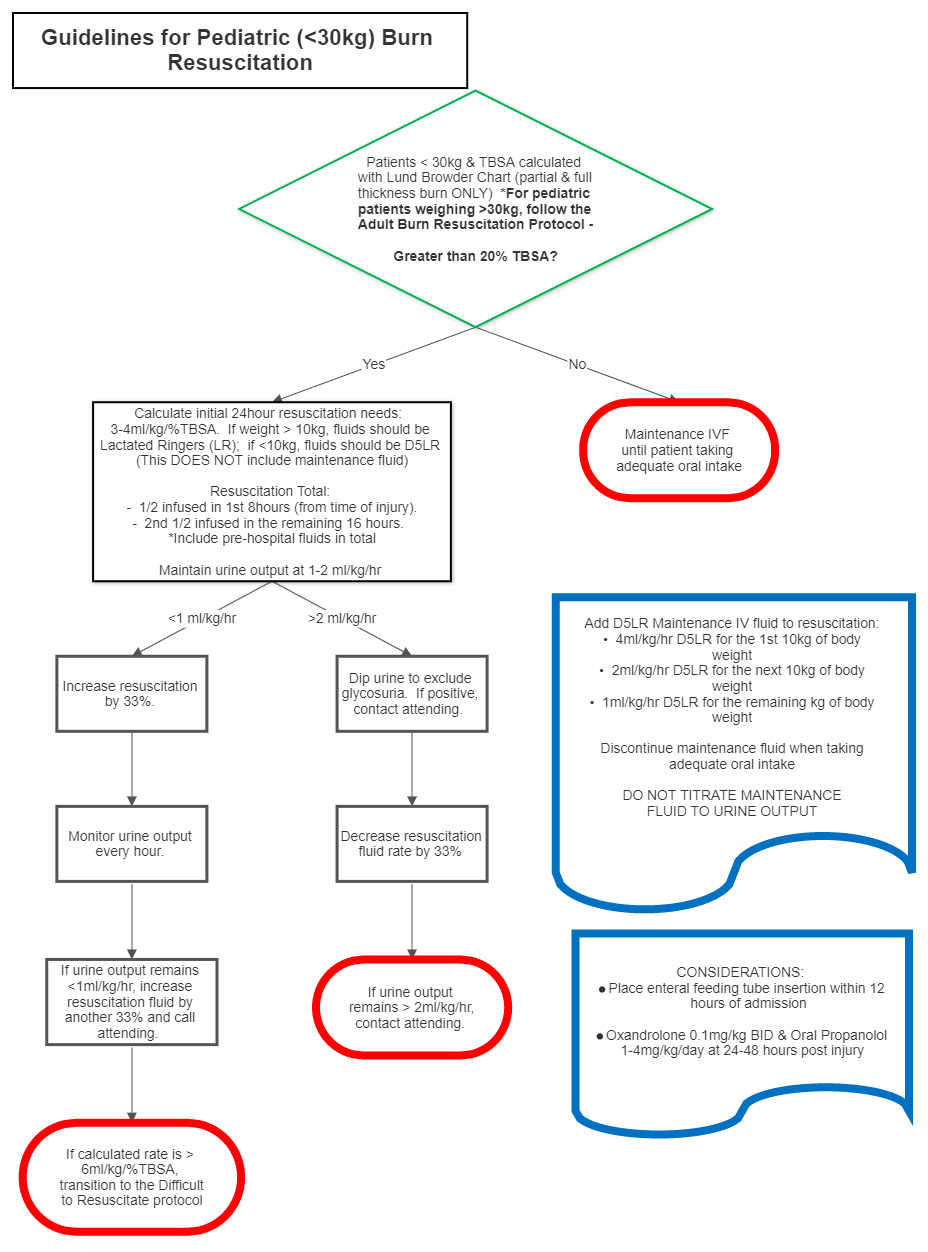
- TBSA less than 20%
- Maintenance IVF only until the patient is taking adequate oral
- TBSA greater than or equal to 20% and weight less than 30kg
- Calculate initial 24 hour resuscitation fluid needs. If weight >10kg, fluid should be Lactated Ringers (LR), if <10kg, fluid should be D5LR
- 3-4 ml x weight in kg x %TBSA
- Administer half of calculated amount over the first 8 hours post burn *
- Administer remaining half of calculated amount over the next 16 hours *
- Fluids administered pre-hospital should be included in 24 hour total resuscitation fluid calculation
- *Note: Hourly fluid resuscitation rate is titrated to urine output; see below.
- In addition to burn resuscitation fluid requirements, also infuse maintenance IVF:
- 4ml/kg/hr D5LR for the first 10kg of body weight
- 2ml/kg/hr D5LR for the next10kg of body weight
- 1ml/kg/hr D5LR for the remaining kg of body weight
- *Note: DO NOT titrate maintenance fluids
- Target urine output is 1-2ml/kg/hr.
- If urine output is less than 1ml/kg/hour:
- Increase resuscitation fluid infusion by 33%
- Monitor urine output on an hourly basis
- If urine output remains <1ml/kg/hr, increase resuscitation fluid infusion by another 33%, and call Burn Attending
- If calculated fluid rate is >6ml/kg/%TBSA, transition to Difficult to Resuscitate Protocol.
- Example: If resuscitation fluid rate is 100ml/hour and urine output is <1ml/kg/hr, increase resuscitation fluid infusion to 133ml/hr. If after one hour, urine output remains <1ml/kg/hr, increase resuscitation fluid infusion to 177ml/hr.
- If urine output is greater than 2 ml/kg/hour:
- Dip urine to exclude glycosuria. If positive, call burn attending
- Decrease resuscitation fluid infusion by 33%
- Continue to monitor urine output on an hourly basis
- If urine output remains >2ml/kg/hr for 2 consecutive hours, call the burn attending
- 3-4 ml x weight in kg x %TBSA
- Place enteral feeding tube within 12 hours of admission
- Calculate initial 24 hour resuscitation fluid needs. If weight >10kg, fluid should be Lactated Ringers (LR), if <10kg, fluid should be D5LR
- TBSA greater than or equal to 20% and weight greater than or equal to 30kg REFER TO THE ADULT FLUID RESUSCITATION PROTOCOL
Burn Resuscitation - Pediatric Guidelines
exp date isn't null, but text field is
Documentation must include patient’s TBSA affected using Lund-Browder diagram (including only partial and full-thickness burns) and a weight in kilograms prior to initiating the protocol. For patients >30kg, follow the ADULT BURN RESUSCITATION Protocol.
- Check serum sodium and potassium every 6 hours on the second day post-injury. Adjust type of fluid by the serum sodium level
- After 24 hours of crystalloid infusion, if fluid requirements remain high, consider changing to 5% albumin. Changing to 5% albumin will only be done at burn service attending physician’s
- The goal is to decrease resuscitation fluid rate to one half of the rate infused over the previous 16 hours. IVF rate is estimated based on patient’s weight, TBSA burned, response to resuscitation, and estimated losses (seek Burn Attending input on calculating estimated losses)
- Patients <30 kg, the urine output goal remains 1-2ml/kg/hour
- Start oxandrolone 0.1mg/kg BID and beta-blockade with oral propranolol 1- 4mg/kg/day