Pediatric Difficult to Resuscitate Protocol - Burns
exp date isn't null, but text field is
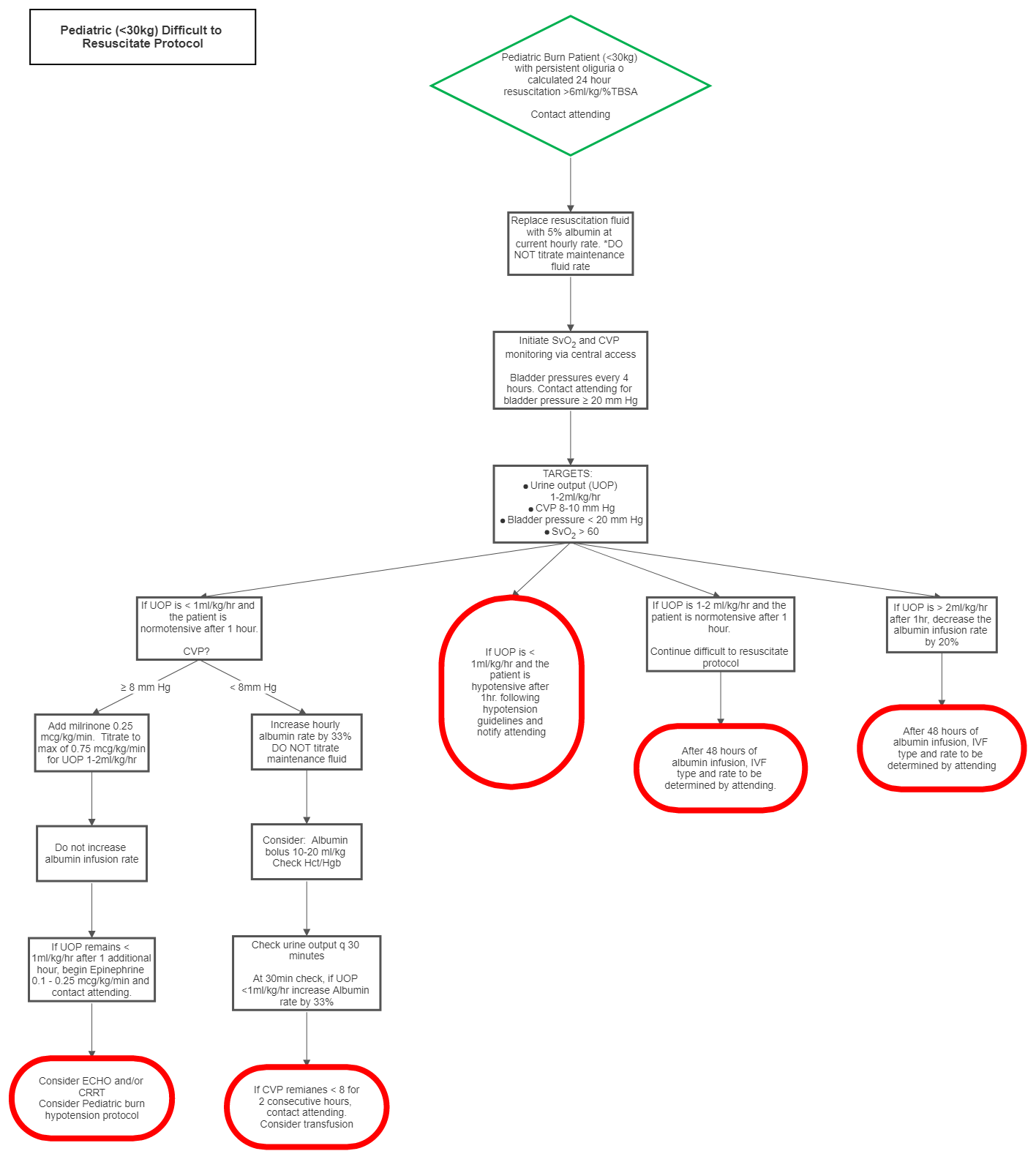
In patients <30kg with persistent oliguria and estimated fluid resuscitation >6ml/kg/%TBSA, switch from Lactated Ringers (LR) infusion to 5% albumin (isotonic premixed 5% albumin or 200ml of 25% albumin in 800ml LR at the previous resuscitation fluid rate.
Note: For patients greater than 30kg, use ADULT DIFFICULT TO RESUSCITATE PROTOCOL.
- Contact burn attending
- Initiate 5% albumin infusion at current resuscitation fluid rate. DO NOT titrate maintenance fluids
- Initiate CVP and SvO2 monitoring via central access. Monitor bladder pressure every 4
- Contact burn attending for bladder pressures ≥20mmHg
- Targets
- Urine output: 1-2 ml/kg/hr
- SvO2: ≥60%
- CVP: 8-10mmgHg
- Bladder pressure: <20mmHg
- If urine output is 1-2ml/kg/hr after 1 hour and the patient is normotensive, continue difficult to resuscitate protocol. Every attempt should be made in minimize fluid administration while maintaining organ
- If urine output >2ml/kg/hr after 1 hour, decrease the albumin infusion rate by 20%.
- After 48 hours of albumin infusion, IVF type and rate to be determined by burn attending
- If urine output is less than 1ml/kg/hr and the patient is hypotensive after 1 hour, follow hypotension guidelines and notify burn attending
- If urine output is less than 1ml/kg/hr and the patient is normotensive after 1 hour
- CVP = <8mmHg
- Increase albumin infusion rate by 33%
- Check hemoglobin & hematocrit
- Consider albumin bolus of 10-20ml/kg
- Check urine output every 30 minutes
- If urine output = <1ml/kg/hr at q30 min assessments, increase albumin infusion rate by 33%
- If CVP remains <8 for 2 consecutive hours, contact burn attending & consider transfusion
- CVP = ≥8mmHg
- Add milrinone 0.25 mcg/kg/min. Titrate to a max of 0.75 mcg/kg/min for UOP 1- 2ml/kg/hr
- DO NOT increase albumin infusion rate
- If urine output remains <1ml/kg/hr after 1 additional hour, add epinephrine 0.1mcg/kg/min and contact burn attending. Titrate to a maximum dose of 0.25mcg/kg/min
- Consider ECHO, CRRT
- Consider hypotension protocol
- CVP = <8mmHg
- If CVP, SvO2, and urine output reach goal, stop increasing fluids and contact burn attending
- If the patient becomes hypotensive along with urine output <1ml/kg/hr, follow the pediatric burn hypotension guidelines, and notify burn attending
- After 48 hours, infusion of albumin should be titrated down. IV fluid type and rate will be determined and ordered by burn attending