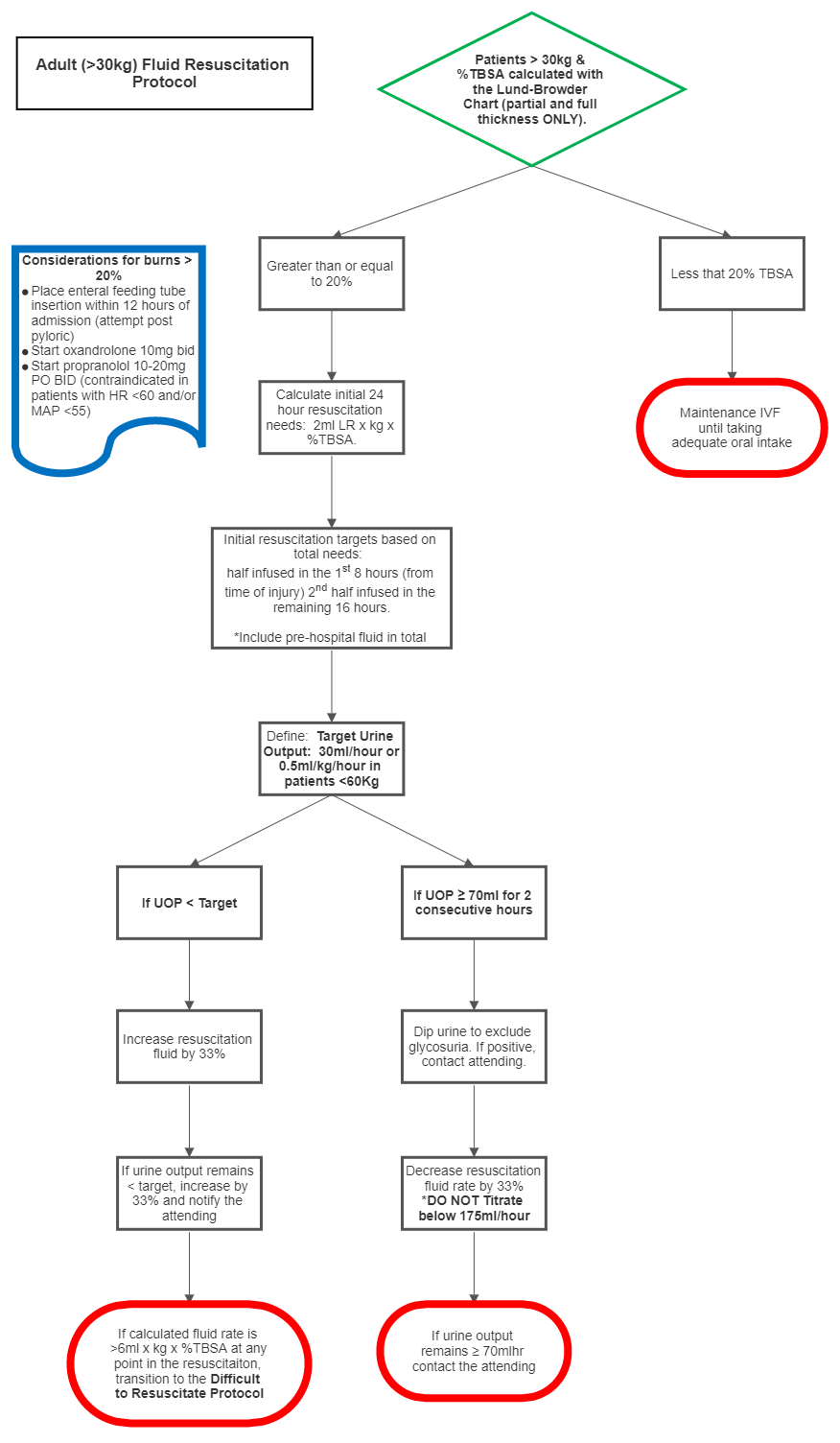
- TBSA less than 20%
- Maintenance IVF only, until the patient is taking adequate oral intake.
- TBSA greater than or equal to 20% and weight greater than or equal to 30kg
- Calculate estimated fluid needs:
- 2cc of LR x weight x TBSA (can increase to 4cc depending on urine output):
- Administer half of calculated amount over the first 8 hours post burn
- Administer half of calculated amount over next 16 hours
- If urine output less than 30cc/hour OR 0.5ml/kg/hr for patients <60kg:
- Increase LR infusion by 33% of the hourly calculated fluid requirement
- If urine output greater 70 cc/hour for two consecutive hours:
- Dip urine to exclude glycosuria
- Decrease LR infusion by 33% of the hourly calculated fluid requirement
- Do not decrease IVF rate below 175cc/hr.
- 2cc of LR x weight x TBSA (can increase to 4cc depending on urine output):
- Calculate estimated fluid needs:
- Place enteral feeding tube as soon as possible for all burns greater than or equal to 20% TBSA
- Consider Esophageal doppler monitor for intubated patients with TBSA >/= 30%, age >50, and/or inhalation injury to measure fluid status and cardiac output. Swan-Ganz catheter placement should only be used as last resort on patients who are not responding to fluid resuscitation and other methods of measurement have failed.
- At 12 hours post burn injury, assess IVF administered and calculate the projected 24 hour total IVF if fluid rates are kept constant. If the projected 24 hour IVF requirement exceeds 6cc/kg/%TBSA burn then switch to the difficult fluid resuscitation guideline (see below.)
Resuscitation - Adult Burn Guideline
exp date isn't null, but text field is
Documentation must include patient’s TBSA burn using Lund-Browder diagram (including only partial and full-thickness burns) and a weight in kilograms prior to initiating the protocol.
- If urine output falls below the low limit (<30ml or 0.5ml/kg/hr whichever is the smaller number) for one hour, increase the current IVF infusion rate by 33% of the calculated hourly requirement.
- If urine output falls below the low limit for a second consecutive hour, increase the current IVF infusion rate by 33% of the calculated hourly requirement.
- If urine output remains below target for a third consecutive hour, notify the burn physician
- Serum sodium and potassium must be checked every 12 hours on the second burn day.
- Adjust type of fluid according to the serum sodium level.
- After 24 hours of crystalloid, if fluid requirements high, consider 5% albumin infusion
- In the second 24 hours, all patients should receive crystalloid or colloid sufficient to maintain urine output and to maintain parameters of perfusion including lactate, pulse pressure variation, and cardiac output. Infusion rate will often be at a maintenance rate plus adjustment for losses of fluid into the burn wound.
- After 24 to 36 hours, providers can cut fluids by 1/3 if the patient continues to make adequate urine.
- One may decrease fluids again by 1/3 for hours 36 to 48 (assuming urine output does not drop off).
- Colloid can be given after initial crystalloid resuscitation (5% albumin at 0.3 to 0.5 mL/kg per % TBSA over 24 hrs)
- If the patient is greater than 30 kg, urine output goal is 30ml/hour (about 0.5ml/kg/hr) (maximum 70cc/hr)
- If the patient less than or equal to 30 kg, urine output goal of 1 cc/kg/hour (maximum 2cc/kg/hr)
- OXANDROLONE
- For burns greater than 20% TBSA, start oxandrolone 10 mg oral twice daily.
- Monitoring liver function tests weekly
- Consider dose reduction to 5mg BID for elderly (>56y/o) or poor renal function
- BETA-BLOCKERS
- Start Propranolol 10-20 mg PO BID (contraindicated in patients with HR< 60 and MAP <55)
- Titrate as tolerated to a maximum dose of 1-4mg/kg/day (Max 640mg/day)
- Dosing can be divided BID or TID