{kind=link}
{kind=link}

Hepatic Trauma (BHT) - Blunt
exp date isn't null, but text field is
- Liver injury occurs in approximately 5% of trauma admissions
- MVC is most common etiology for BHT
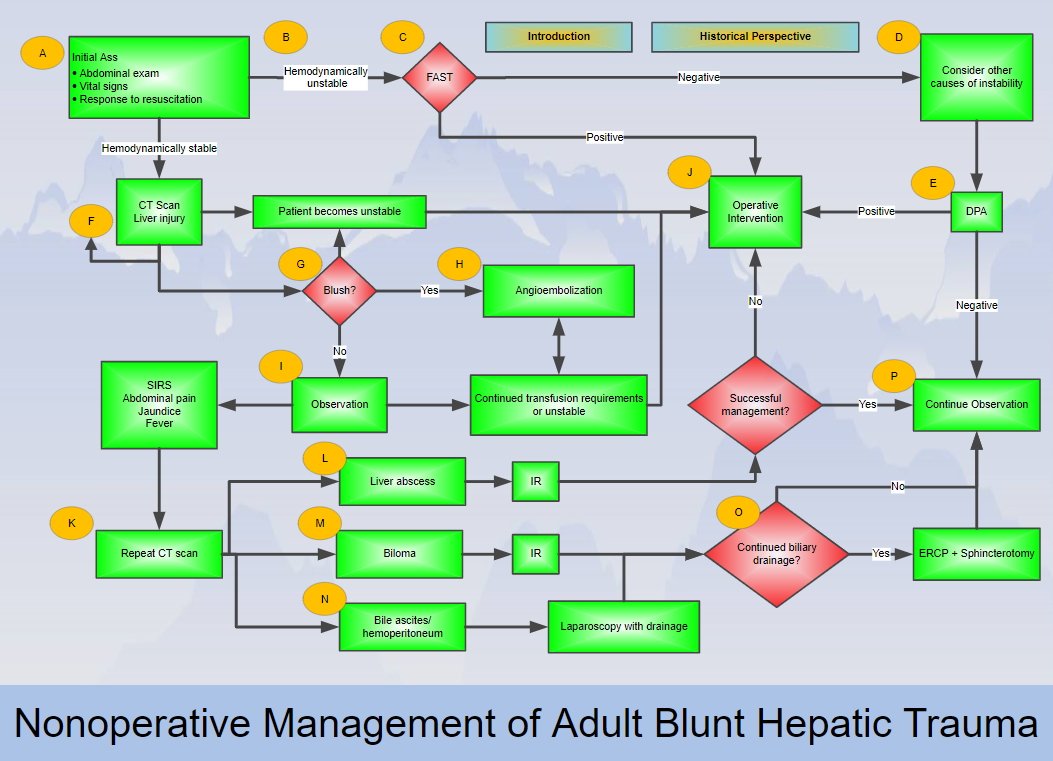
- FAST is key to rapid diagnosis of hemoperitoneum in the unstable patient but unreliable in determining grade of liver injury
- CT scan allows further evaluation and grading of hepatic injury in a stable patient
- Blunt hepatic injury typically traverses along segments of liver
- Hepatic veins most commonly injured in BHT
- Non-operative management has become standard for stable patients with BHT (approx. 85% of patients w/BHT are stable) with embolization and/or drainage by IR an important adjunct
- High-grade injury, large hemoperitoneum, contrast extravasation, and pseudoaneurysm are not contraindications for non-operative management, however at higher risk for non-op failure
- Complications can include: compartment syndrome, bile leak, abscess, hemobilia, delayed hemorrhage, devascularization
- No evidence to keep stable patients on bed rest
- No evidence for routine f/u CT scans, only scan if clinical change
- Most patients can resume full activity in 1 month (consider f/u CT scan for grade III-V before resume full activity) - (No level I evidence, based on level II and III data)
|
Grade* |
Description |
|
|
I |
Hematoma |
Subcapsular, <10% surface area |
|
Laceration |
Capsular tear, <1cm parenchymal depth |
|
|
II |
Hematoma |
Subcapsular, 10-50% surface area |
|
Laceration |
Capsular tear, 1-3cm parenchymal depth, <10cm length |
|
|
III |
Hematoma |
Subcapsular, >50% surface area or expanding Ruptured subcapsular or parenchymal hematoma Intraparenchymal hematoma >10cm or expanding |
|
Laceration |
>3cm parenchymal depth |
|
|
IV |
Laceration |
Parenchymal disruption involving 25-75% of hepatic lobe or 1-3 Couinaud’s segments within a single lobe |
|
V |
Laceration |
Parenchymal disruption involving >75% of hepatic lobe or >3 Couinaud’s segments within single lobe |
|
Vascular |
Juxtahepatic venous injuries (i.e. retruhepatic vena cava/central major hepatic veins) |
|
|
Vascular |
Hepatic avulsion |
|
*Advance one grade for multiple injuries up to Grade III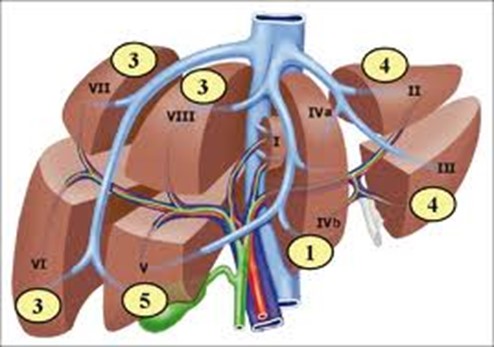
Day 2-3 after admission for Liver AIS ≥ 4: Consider HIDA scan to rule out bile leak. If positive laparoscopic washout with drain placement. If negative repeat only as indicated. Consider ERCP if bile drain output remains >200cc/day after a week.